
.png)
.png)
.png)
.png)












 3 hours ago
2
3 hours ago
2
ARTICLE AD BOX
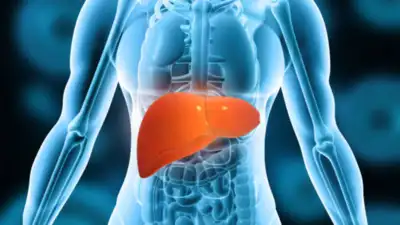
Two of the most prevalent causes of chronic liver injury in the world are hepatitis and fatty liver disease. Subtle symptoms are frequently missed, which can postpone diagnosis and treatment, even though both conditions can develop quietly over years.
Preventing advanced liver disease, such as cirrhosis and hepatocellular carcinoma, requires early detection.
Definition and pathophysiology of fatty liver disease
Excessive fat accumulation (greater than 5%) in hepatocytes is an indicator of fatty liver disease, also referred to medically as hepatic steatosis. It falls into the following categories:
Fatty liver disease associated with alcohol (AFLD)
NAFLD, also known as non-alcoholic fatty liver disease, Steatotic liver disease linked to metabolic dysfunction (MASLD)Since obesity, type 2 diabetes, and metabolic syndrome are on the rise, MASLD is becoming more and more common.
It develops into metabolic dysfunction-associated steatohepatitis (MASH), a condition that can result in cirrhosis, fibrosis, and liver cancer, when linked to hepatic inflammation and injury.Insulin resistance, which encourages lipolysis and the influx of free fatty acids into the liver; oxidative stress and mitochondrial dysfunction; and the production of inflammatory cytokines, such as TNF-α and IL-6, are all part of the pathogenesis including Dysbiosis of the gut microbiota, which increases hepatic inflammation and endotoxemia.
Hepatitis: Inflammatory liver injury
Hepatitis is an inflammation of the liver that can have a number of causes.Hepatitis A, B, C, D, and E are viral autoimmune hepatitis. Drug-induced liver injury (DILI), which includes antibiotics, herbal remedies, and paracetamol. Hepatitis caused by alcohol Hemochromatosis, Wilson's disease, and alpha-1 antitrypsin deficiency are metabolic causes.While acute hepatitis may be symptomatic, chronic hepatitis often presents insidiously and is detected only on routine blood tests or when complications arise.
Common and ignored hepatitis and fatty liver symptoms
Numerous initial signs of liver disease are vague and commonly confused with other gastrointestinal or systemic issues. Some symptoms that are frequently overlooked or underrecognized are listed below:
- Chronic fatigue: Usually dismissed as stress-related or anemia-related, liver disease causes fatigue through altered neurotransmission and systemic inflammation.
- Mild right upper quadrant pain: Often mistaken for gallbladder disease, gastritis, or musculoskeletal pain, this pain may be a sign of hepatomegaly or hepatic capsule stretching.
- Unexplained itching (Pruritus): Often precedes jaundice and is misdiagnosed as skin disorders; particularly observed in cholestatic hepatitis (e.g., hepatitis C, autoimmune cholangitis).
- Brain fog and sleep disturbances are brought on by early hepatic encephalopathy or cytokine-related cognitive effects. Patients complain of memory issues, trouble focusing, or irregular sleep patterns.
- Muscle wasting and weight loss: Sarcopenia, or subtle muscle loss, is frequently disregarded, particularly in obese patients; it may indicate the development of advanced fibrosis or cirrhosis.
- Skin and nail changes: Chronic hepatitis may cause palmar erythema, spider angiomas, and leukonychia (white nails); MASLD is associated with metabolic dysfunction and hyperpigmentation and acanthosis nigricans.
- Sexual dysfunction and irregular menstruation: Frequently underreported and overlooked during clinical evaluation, this condition is observed in advanced liver disease as a result of altered sex hormone metabolism.
- Low-grade fever is frequently misdiagnosed as a viral disease or urinary tract infection, and it is common in autoimmune or drug-induced hepatitis.
Diagnosis and evaluation
Elevated ALT, AST, or GGT are frequently seen in routine liver function tests (LFTs), but these tests are insufficiently sensitive or specific to identify fatty liver or hepatitis. To measure liver fat and fibrosis, imaging techniques like MRI-PDFF, elastography (FibroScan), and ultrasound are useful.
The gold standard for staging autoimmune hepatitis or MASH is still liver biopsy.Immunoglobulin levels, autoimmune markers (ANA, SMA, LKM), and viral serology are critical for hepatitis. Serum ferritin, lipid profile, and HbA1c should all be part of the metabolic evaluation.In conclusion, hepatitis and fatty liver frequently exhibit mild, nonspecific symptoms that are simple to ignore, particularly in patients with coexisting metabolic disorders. Raising patient and clinician awareness of these symptoms may help prevent irreversible liver damage by enabling earlier diagnosis and treatment. Maintaining a high index of suspicion and conducting routine screening are still essential, especially in high-risk populations.By Dr. Pavan Dhoble, Consultant, Gastroenterology, P. D. Hinduja Hospital & Medical Research Centre, Mahim







 English (US) ·
English (US) ·